RESPECT. DIGNITY. INCLUSION.
Support the fight for disability rights.

Promoting and protecting the human rights of people with intellectual and developmental disabilities and actively supporting their full inclusion and participation in the community throughout their lifetimes.
With your help, we are working every day to build a future of inclusive work, play, worship, community, travel, and more.
LOCAL CHAPTERS
DRIVING CHANGE AND PROTECTING THE RIGHTS OF INDIVIDUALS WITH DISABILITIES
NATIONAL AND COMMUNITY PROGRAMS





November 5, 2024, is Election Day and there are so many elections happening at the local, state, and federal levels. The people who get picked to run the government can make decisions that have a big impact on the lives of people with disabilities and their families. If you don’t vote, then you don’t get a say in what happens. Use our free resources to check if your voter registration status, register, and to make sure you have the information you need to make your vote count the next time you cast a ballot.
Whether you are a parent, educator, service provider, or non-attorney advocate, The Arc@School’s Advocacy Curriculum provides the basic information needed to navigate the special education system. Learn about early intervention services, individualized education programs, Section 504, and more. We also have a new Advocacy Curriculum in Spanish!


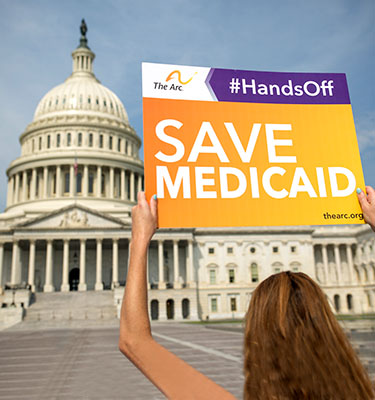
The Arc fights every day to protect civil rights and access to vital programs, such as Medicaid, for those with intellectual and developmental disabilities (IDD). But we can’t do it alone! We need the help of people with IDD, their families, and allies of the cause.
Sign up today to receive updates on our movement, take action, and make a difference in the lives of people with disabilities.





Will you pledge to vote this November?